Audit Questionnaire & Score
| 1. How often do you have a drink containing alcohol? | |
| 2. How many drinks containing alcohol do you have on a typical day when you are drinking? | |
| 3. For FEMALES how often do you have 4 or more and for MALES how often do you have 5 or more drinks on one occasion? | |
| 4. How often during the last year have you found that you were not able to stop drinking once you had started? | |
| 5. How often during the last year have you failed to do what was normally expected from you because of drinking? | |
| 6. How often during the last year have you needed a first drink in the morning to get yourself going after a heavy drinking session? | |
| 7. How often during the last year have you had a feeling of guilt or remorse after drinking? | |
| 8. How often during the last year have you been unable to remember what happened the night before because you had been drinking? | |
| 9. Have you or someone else been injured as a result of your drinking? | |
| 10. Has a relative, friend, doctor, or other health worker been concerned about your drinking or suggested you cut down? | |
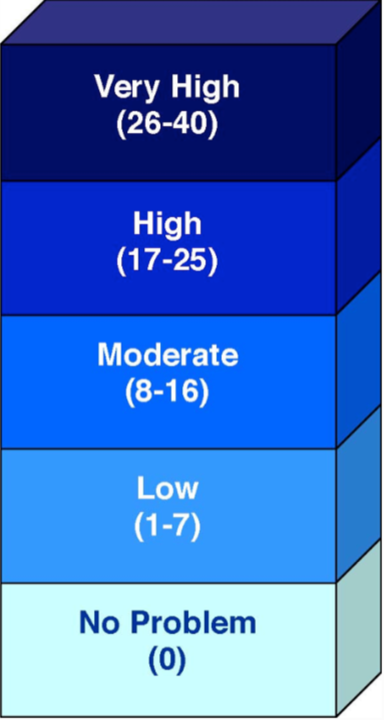
| Your Audit Score: | |
The AUDIT Questionnaire was developed by the World Health Organization to evaluate a person’s use of alcohol and the extent to which drinking is a problem. Higher scores typically reflect more serious problems.
Where Does Your Audit Score Fit In?